Covid-19: What are the Facts? Does Anybody Know?
Following is a dissertation on what I have come to understand about Covid-19, based upon my own research into what others are finding and saying, as well a basic biological facts that have been undisputed for decades.
What is Covid-19 and why does it divide us as it does? Covid-19 is the designation given to a virus that came onto the world stage in 2019, showing up first in Wuhan Province in China and then spreading around the world thanks to our global economy and air travel. The Covid-19 virus is a variation of the corona virus. Every flu season has a typical cycle to it. It generally begins in early to mid-autumn with the arrival of the rhinovirus. As the winter encroaches on us there will generally be an A or B type strain of influenza that makes an appearance, and as we approach spring and into the early summer we deal with some variant of a corona virus.[1] This happens every year. Each strain of each virus will be a variation of previous strains of the previous years’ viruses with different characteristics which means that we will all be susceptible to catching any or all of these viruses each year. It also means that we will all have a degree of an immune response to each of the viruses every year.
Our bodies catalog every virus that it battles over the years and uses this information to identify and attack all future viruses that it comes into contact with. The identifying markers that the body uses to identify the virus are locked into the DNA or RNA of the virus.
This gets a little technical now. Covid-19 does not have DNA, it has RNA. In the laboratory the RNA is converted to DNA in order for the PCR (polymerase chain reaction) test to identify it. There are several steps to actually test for Covid-19, which include numerous cycles of amplifying the test matter and adding primers and probes to make the virus visible to detection equipment via fluorescence. So this means that, in order to make a positive diagnosis of Covid-19, the lab must have a sample of the RNA/DNA for the test to match to. But do they?
According to the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel[2], apparently not. “Since no quantified virus isolates of the 2019-nCoV are currently available, assays designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA (N gene; GenBank accession: MN908947.2) of known titer (RNA copies/μL) spiked into a diluent consisting of a suspension of human A549 cells and viral transport medium (VTM) to mimic clinical specimen.”(emphasis added) This means that scientists took the RNA identifiers of previous corona virus outbreaks and used those to create a test to indicate the presence of Covid-19. Does this pass muster scientifically? It depends on what your goals are. If you are intending to show that the test subject has been exposed to a corona virus, then yes, absolutely. If you are intending to show that the test subject has been exposed to Covid-19, then no, it does not meet the standard necessary for confirmation. This report originated in February of 2020, but the latest update appears to have been in July, with no alteration to this information regarding the isolation of a specific Covid-19 virus.
Further to this point, “the FDA authorized IVDs (in-vitro diagnostic) based on available data from contrived samples generated from a range of SARS-CoV-2 material sources (for example, gene specific RNA, synthetic RNA, or whole genome viral RNA) for analytical and clinical performance evaluation. While validation using these contrived specimens provided a measure of confidence in test performance at the beginning of the pandemic, it is not feasible to precisely compare the performance of various tests that used contrived specimens because each test validated performance using samples derived from different gene specific, synthetic, or genomic nucleic acid sources.”[3] (emphasis added) Again, they used “contrived specimens” to create this testing process and to validate its performance, something akin to using a student’s test as the key to mark that student’s test and finding that the answers are all correct.
This type of testing is illogical at best. Sure, you can say that you have found a corona virus, but which one? You have modeled the test on multiple samples of virus without the data for Covid-19, so how can you definitively say that you have found Covid-19? Quite simply, you can’t.
There is typically a “gold standard” for medical testing to ensure that the testing is precise and accurate; according to Dr. Sanjaya Senanayake in an interview with ABC television, “If we had a new test for picking up [the bacterium] golden staph in blood, we’ve already got blood cultures, that’s our gold standard we’ve been using for decades, and we could match this new test against that. But for COVID-19 we don’t have a gold standard test.”[4] Jessica C. Watson, a GP and National Institute for Health Research doctoral research fellow agrees, “No test gives a 100% accurate result; tests need to be evaluated to determine their sensitivity and specificity, ideally by comparison with a “gold standard.” The lack of such a clear-cut “gold-standard” for Covid-19 testing makes evaluation of test accuracy challenging.”[5]
Furthermore, even the CDC states that “Positive results are indicative of active infection with 2019-nCoV but do not rule out bacterial infection or co-infection with other viruses. The agent detected may not be the definite cause of disease.”[6](emphasis added) The CDC, in the same document, also states that “Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.” This means that the CDC recognizes the possibility of false positive results. This test is not a definitive diagnosis, nor should it be used as such, but our “medical professionals” and politicians are basing all of their recommendations and restrictions on the results of a test that even the CDC does not fully believe in.
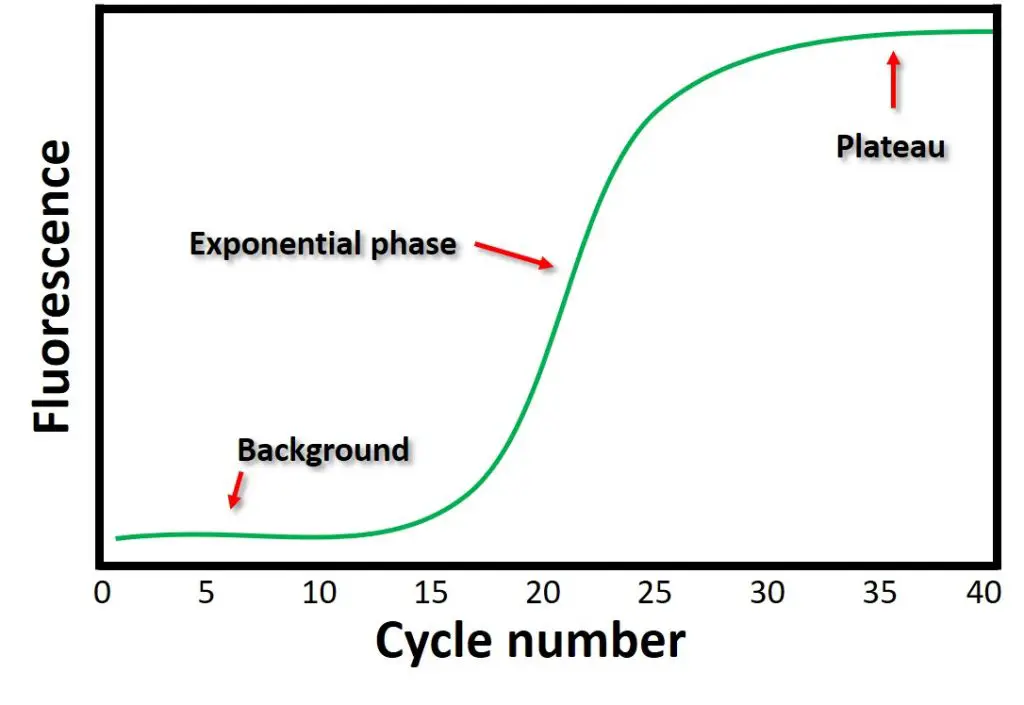
Another indication of the weaknesses of using the PCR test as a diagnostic tool for Covid-19 is the amplification cycles. If the PCR test was ideal for testing for Covid-19, the amplification cycles required to detect the virus should be noted as soon as virus is detected. This would indicate the level of infection that can be found on the sample.[7] This is not how the test is administered though.
According to the following graph[8], the highest likelihood of finding a true positive result of any consequence to the health or communicability of an individual would be found in the range of approximately 15-25 amplification cycles. Anything before 15 cycles would not be detectable except in the most severe infections, anything beyond 30 is grasping at straws. According to MIT, “Most tests, like the Broad Institute test used by MIT, use a 40-cycle protocol. If the virus isn’t detected within 40 amplification cycles, the test result is negative. If viral RNA is detected in 40 cycles or less, the PCR machine stops running, and the test is positive. Because you received a positive result, we know that the test detected the virus in your sample by the time it reached its 40-cycle limit.”[9] “A positive test that comes back positive in 20 cycles contains a greater amount of virus than one requiring 40 cycles. Right now, we just call both results “positive.” But it’s obvious that the first sample came from an individual with a higher viral load. And the greater the viral load, the more contagious the patient is likely to be.”[10]
Now, just as an example, let me point out how much of a difference there is between 25, 30 and 40 amplification cycles.
Let’s start with one item and amplify it once, making it two items. Amplify it again and it becomes four items. Amplify that yet again and it becomes eight items. That is three amplification cycles. Do that to 25 cycles and you have 33,554,432 items. If you keep going to 30 cycles you end up with 1,073,741,824 items. Now this is already at the top of the recommended number of cycles for this type of test. As I said earlier, any more than this is grasping at straws. Now if you go to 40 cycles you get 1,099,511,627,776 items. In 15 cycles we have gone from 33 million items to over one trillion.
Most of us cannot comprehend those numbers, so I’ll add this to bring it into context. One million seconds will take over a week and a half to lapse. One billion seconds would take almost 32 years, and one trillion seconds will take 31,688 years to lapse.[11] There is a BIG jump from million to billion and an even bigger jump from billion to trillion. This is all to say that 40 amplification cycles is practically squeezing a positive result out of a sample.
So what does this mean? It means that scientists are going to extreme lengths to obtain any significant number of positive test results from these PCR tests.
Now let’s look at these test results, get ready for a lot of numbers. According to the Government of Canada[12], as of November 13, 2020 there have been 10,228,547 Coid-19 tests conducted in Canada. Realize that this is the number of tests, not the number of people who have been tested; there is a difference. Of those tests, 287,318 came back positive, which is a 2.8% positivity rate. There have been 10,828 deaths “with” Covid-19 (I will explain the “with” later). That means that of the people that have tested positive for Covid-19 in Canada, 3.8% have died. Unfortunately, due to the way things are reported it is hard not to conflate data here, so please bear that in mind when you realize that of the 10 million plus tests that have been conducted, essentially 0.11% of those tests resulted in someone’s death (I know that is not quite accurately stated but it’s the best we can do when the country decides to make case count more important than hospitalization or death count).
If we look at the recovery numbers we see that of the 287,318 positive cases, 230,646 have recovered, which is just over 80% of the positive test results did not end up in death, to this point. Let’s add 80% of the 45,844 active cases to the recovery number and we see that we can project that of the 287,318 positive cases, we can expect that 267,321 will recover from the current number of positive cases in Canada, which is a 93% recovery rate.
If we look more closely at the death figures we will see that in the nine months from March till now in mid-November we have lost 10,828 citizens who have died “with” Covid-19. The current population of Canada is projected at 37,742,154[13] as of November 14, 2020. I’m just going to make that 37,750,000 to make things easy. We have lost 0.02868% of our population to causes “related to” Covid-19 (again with the quotation marks – I’ll get to that, be patient).
Now every death is a loss, but we need to put emotions aside when dealing with matters of national or provincial interest. The reality of things is that people die, every day, for various reasons and from various causes. Over the last 20 years Manitoba has averaged an annual death rate of 10,281 people[14], and this year is so far pegged at 11,266, with the last four years all having death rates of over 11,000 people in this province. This chart indicates that the totals are taken from July 1 to June 30 of, presumably, every year, so we are on track to have more deaths this year than other years.
By the way, our current death toll of those who died “with” Covid-19 in Manitoba is 152. Other numbers from Manitoba as of November 14, 2020 are, 307,056 tests, 10,453 positives, 228 hospitalized which I assume includes the 34 in the ICU.[15] That’s a 3.4% positivity rate on testing. A population of 1.272 million people lost 0.01% of our population to Covid-19.
Now, about those quotation marks around “with” and “related to”. For those who were paying attention in the early days of Covid-19, the news would report that X number of people died of or from Covid-19. Probably around early to mid-summer I noticed that nobody died of or from Covid-19, but now everybody died “with” Covid-19 or from issues “relating to” Covid-19. Why is this worthy of note?
Well, when you tell people that someone died from a heart attack, or pneumonia or Covid-19, you are stating what the cause of death was. When you say that someone died “with” Covid-19, that changes the narrative, but in a way that most people likely won’t consider. If someone dies in the hospital having been admitted only with symptoms indicating Covid-19, and has tested positive for the virus, then it is safe to say that said person died from Covid-19.
If, however, a guy comes in having been hit by a bus, with internal bleeding and severe head wounds, but he tests positive for Covid-19, and he dies, then he died “with” Covid-19. As I mentioned earlier, for the last several months everybody that has dies has died “with” Covid-19. Make of it what you will but words are important, all reporting seemed to have made this same change around the same time and this has been a consistent announcement for months.
Now keep in mind that before Covid-19, there was never a campaign to pursue or mandate wide spread testing of the population for any viral infection, whether they are symptomatic or not. We have seen the number of tests increase by approximately 14 times from March of 2020[16](chart), from about .16 per thousand to a peak of about 2.25 per thousand people. This translates to about 6,040 people per day in March to 84,938 per day in October, based on the prior used figure of 37,750,000 people in Canada. So have our cases jumped by a multiplier of 14 as well? Well, no.
I like to use graphs when possible to show what is going on at a glance. The chart below[17] indicates that our case count has increased by a multiplier of about 10, but that is only really since about the end of September, the numbers were mostly flat before that, with incremental rising, but not exponentially rising numbers. Do you know what else happened at the end of September? Manitoba’s Dr. Brent Roussin mandated that masks must be worn indoors in the City of Winnipeg.[18] This was later expanded to include all of Manitoba.
 Now I want you to stop and think about cause and effect. If
the number of positive Covid-19 tests started to rise towards the end of
summer, when people have spent a lot of time outside, but likely still social
distancing, and there was no corresponding rise in cases prior to the end of
September, what could that mean? What changed? Is it possible that wearing a
mask can actually make you sick? There is quite a bit of research on that
actually, but it has also been shown that wearing a mask seems to have no effect
on keeping you healthy.
Now I want you to stop and think about cause and effect. If
the number of positive Covid-19 tests started to rise towards the end of
summer, when people have spent a lot of time outside, but likely still social
distancing, and there was no corresponding rise in cases prior to the end of
September, what could that mean? What changed? Is it possible that wearing a
mask can actually make you sick? There is quite a bit of research on that
actually, but it has also been shown that wearing a mask seems to have no effect
on keeping you healthy.
The CDC released a report in July[19] which included data on how much people wore masks in both a group of Covid-19 positive people and a Covid-19 negative control group. This report was widely reported to have shown that the majority of people who wore masks contracted Covid-19. I don’t agree with that conclusion, but I did find something else in the numbers that is less debatable but just as enlightening.
If you look at page 1261 of the report there is a table at the top of the page. At the bottom of this table are the numbers that people cited for the above mentioned claim. But if you look at the numbers of the infected people and the numbers of the non-infected people across the columns, focusing on how much they wore a mask you will see that the numbers of the infected and non-infected are very similar regarding how much they wore their masks. This tells me that masks are not effective protection against the Covid-19 virus. There is about a 50% chance that you will get sick whether you wear a mask or not, regardless of how much you wear a mask.
There are, again, numerous studies that have shown that wearing a face mask is not effective against the Covid-19 virus, several are cited in this article,[20] which I will not go into detail here, but you can search them all out for yourself. There are also several articles mentioned that claim to prove that masks are effective, but the article also points out why these are not to be trusted.
There is also the matter of correct use of PPE. Believe it or not, PPE, or personal protective equipment, is not something that is designed for the average Joe to use without training. Healthcare professionals, lab technicians and others that use PPE for their work receive specific training on how to put on, use and care for their PPE. Most people on the street do not have that training and as a result, are using their face masks incorrectly, contaminating their face masks repeatedly or are overusing their face masks. This can lead to a higher chance of infections, from either Covid-19 or any other viral or bacterial infection.[21]
Dr. James Meehan, MD, is a doctor from Tulsa, Oklahoma who is part of a group that has filed a lawsuit against the Mayor and the Health Department Executive Director over their mandatory mask mandates. Dr. Meehan has been “warning that mask wearing has “well-known risks that have been well-studied and they’re not being discussed in the risk analysis.” “I’m seeing patients that have facial rashes, fungal infections, bacterial infections. Reports coming from my colleagues, all over the world, are suggesting that the bacterial pneumonias are on the rise.” “Why might that be? Because untrained members of the public are wearing medical masks, repeatedly… in a non-sterile fashion… They’re becoming contaminated. They’re pulling them off of their car seat, off the rear-view mirror, out of their pocket, from their countertop, and they’re reapplying a mask that should be worn fresh and sterile every single time.” Dr. Meehan adds: “New research is showing that cloth masks may be increasing the aerosolization of the SARS-COV-2 virus into the environment causing an increased transmission of the disease…”
In conclusion, Dr. Meehan states: “In February and March we were told not to wear masks. What changed? The science didn’t change. The politics did. This is about compliance. It’s not about science… Our opposition is using low-level retrospective observational studies that should not be the basis for making a medical decision of this nature.”[22]
Notice the mention of aerosolization; what does that mean? We all use products that come in a pressurized can that is released when we press the nozzle on the top. These are referred to as aerosols. This term is also used in the process of spraying paint using pressurized air. An air spray gun has controls on it to control the air flow to get more or less aerosolization of the paint media. This means that the painter can control how large or small the air-carried paint particles are, which allows the painter to get either a faster but poor finish, or a slower but finer paint finish. The smaller the particles are, the better paint finish you end up with. This is attained through higher aerosolization.
Why is this important? Dr. Theresa Tam, Canada’s National Health Officer, recently quietly announced that "The (Covid-19) droplets vary in size from large droplets that fall to the ground rapidly within seconds or minutes near the infected person to small droplets, sometimes called aerosols, which linger in the air under some circumstances."[23] This means that the particles can be very, very small, can linger in the air and can sneak around the gaps of your mask. You know, the gaps by your nose and around the sides. This article[24] states as much: “Although surgical mask media may be adequate to remove bacteria exhaled or expelled by health care workers, they may not be sufficient to remove the submicrometer-size aerosols containing pathogens to which these health care workers are potentially exposed.” This is to say that somebody wearing a mask can still inhale aerosolized contaminants.
Now let’s look again at the previous quote about masks and aerosolization. “Dr. Meehan adds: “New research is showing that cloth masks may be increasing the aerosolization of the SARS-COV-2 virus into the environment causing an increased transmission of the disease…”[25](emphasis added) So if we take these pieces of information all together, we get that there is the likelihood that Covid-19 can be spread through aerosolization of the virus from infected individuals, masks may actually increase the aerosolization of the virus and masks are not effective protection against aerosolized contaminants, indicating that masks may not only be less than effective, but may be adding to the problem.
I also want to take a bit of space here to point out that when one wears a mask, it tends to get wet from their breath and it is very warm as well. History has shown us that warm and wet environments are ideal breeding grounds for bacteria and mould. By using your face masks, especially if you use them repeatedly, you are effectively enclosing your face with a bacteria factory and breathing those bacteria right into your sinuses and down into your lungs with every breath. Again we look at the statements made by Dr. Meehan, ““I’m seeing patients that have facial rashes, fungal infections, bacterial infections. Reports coming from my colleagues, all over the world, are suggesting that the bacterial pneumonias are on the rise.” “Why might that be? Because untrained members of the public are wearing medical masks”[26] Keep in mind that for decades people have been fighting air pollution because we know that the cleaner the air is that a person can breathe, the healthier that person is likely to be. So why would you want to intentionally contaminate every breath you take? It is not good for your health.
Masks are just part of the restrictions that we have dealt with, and we all know that the restrictions in the spring of 2020 were placed on us in order to “flatten the curve”. There was concern about the hospitals getting overwhelmed with infected people. And in hindsight, there may have been value in that as there was not a lot known about the virus at that time and it was a precaution, though one that did violate the basic freedoms of individuals. Now we know a lot more about the virus and how to treat it, but we are still placed under restrictions of movement, commerce and socialization. Is there a basis for this action? We have been hearing that our hospitals are a maximum capacity, that nurses are working long hours and that there are no more beds. That may be true, but this is not an anomaly.
Every year our hospitals are inundated with people during the flu season, from fall all the way through to spring with waves of sick people rising and falling. In February of 2020 (before Covid-19 hit), Dr. Mark Jarrett, who oversees the operation of 23 hospitals in the State of New York, stated that “All the hospitals are taxed with a large flu season and other bugs,” and “Everybody is at maximum capacity,”[27] In 2018 the following was reported in regards to the influx of patients during the regular flu season, “A tsunami of sick people has swamped hospitals in many parts of the country in recent weeks as a severe flu season has taken hold. In Rhode Island, hospitals diverted ambulances for a period because they were overcome with patients. In San Diego, a hospital erected a tent outside its emergency room to manage an influx of people with flu symptoms.”[28] This was due to a regular flu; a recurring phenomenon that strikes with varying severity.
The CDC spoke of the 2018-2019 flu season this way, “CDC estimates that the burden of illness during the 2018–2019 season included an estimated 35.5 million people getting sick with influenza, 16.5 million people going to a health care provider for their illness, 490,600 hospitalizations, and 34,200 deaths from influenza (Table 1). The number of influenza-associated illnesses that occurred last season was similar to the estimated number of influenza-associated illnesses during the 2012–2013 influenza season when an estimated 34 million people had symptomatic influenza illness6.”[29] As of November 16, 2020, according to the CDC, in the U.S. there were 10,984,398 reported cases of Covid-19 and 245,470 deaths, though the accuracy of the number of Covid-19 deaths has been highly disputed. “On August 26, the U.S. Centers for Disease Control and Prevention (CDC) issued a report showing that in 94 percent of the roughly 180,000 deaths that have been attributed to COVID-19, “on average, there were 2.6 additional conditions or causes per death.” “As the CDC report notes, “For 6% of the deaths, COVID-19 was the only cause mentioned.”[30] We do not know what the comorbidities are as they are not reported on, but Covid-19 may have only been what pushed them over the edge of what they had already been dealing with. This is the from/with dilemma again. I suggest that the honest death numbers reside somewhere in the middle.
We need to look at these things rationally. If we take all of this information that I have shared here together, here is the picture that I come away with:
1. Covid-19 is a variation of the seasonal corona virus that we are exposed to every year.
2. The health effects of Covid-19 can be very severe, possibly leading to loss of life in severe cases – the same can be said of the overall flu season for every year in history.
3. The population in general will have an historical immunity at some level, with the elderly and immunocompromised at the highest risk of infection and complications – just like every year.
4. Our hospitals will be filled to capacity with sick people during this pandemic – just like every year.
5. People will die and the best we can hope to do is to do our best to try to get them through and keep them as comfortable as possible when they cannot be saved – just like every year.
We live in an era of 24 hour news, data equipped personal devices that are at our side more than any person that we know, and information gathering capabilities from around the world that has been previously unimaginable. News agencies thrive on ratings, clicks and shares. If the news is not sensationalised then it won’t get the attention that the networks need in order to seem to stay relevant. Modern news agencies would go bankrupt if they started telling us that there is nothing to worry about, nothing to be fearful of. Their very business model is built on the cultivation of fear in society. News agencies are the doomsayers of our modern world, and we just can’t help but to repeatedly check to see what they are saying we should be afraid of now, and with the current 24 hour news cycle, they need to constantly be digging up new information to shovel into our brains and repeating ad nauseum what they have already told us when there is nothing new to report.
We are inundated with bad news all day every day and our brains have stopped listening to the details, which we should listen to and be willing to question. Logical fallacies slip past our mental gate without a second consideration because there is more information pushing them past our gatekeeper faster than he can monitor it. We need to slow down. We need to permit ourselves the luxury of taking in the news only once or twice a day and then take the time to digest what we have heard, weighing it against what we have been told previously and sifting it for half-truths, omissions and logical gaps. We also need to be able to put our emotions on the shelf for a little while and think rationally about all that we are being told. Emotional reactions lead to knee-jerk solutions and bungled opportunities which seldom are of any use to the situation or the people involved.
We are being socially engineered with the Covid-19 restrictions that we are being forced to bear. In the past, if there was an endemic or pandemic we were told to stay rested, eat healthy, get exercise and fresh air – in short to care for your own health. Now we are being told to protect the health of others by retreating from everyone, cover your face and report those that don’t comply. Our leaders are using peer pressure and guilt to force people to comply with the mandates. “If you don’t do this you may get someone else sick, maybe even Grandma”. “It doesn’t matter if you do not feel sick, you might get someone else sick in your ignorance”. And the general public is their cost-free prime enforcement force through tactics of guilt and pubic shaming. “How dare you not protect me! You selfish *$#%!” When did your health become my responsibility? When did my health become yours? Am I responsible to make sure that you eat well, get enough sleep and remain active? Are you responsible for me? No, we are all responsible for our own health and we have no say over whether someone smokes, eats only junk food or remains sedentary day after day. You take care of you and I will take care of me.
Finally, we need to keep perspective. I am a Christian. My faith in a God that is in control and who loves me shapes the very fabric of my being. My life, my health and my future are placed entirely in God’s hands, and they are all safe there. Does this mean that I and all of the members of my family will remain safe from Covid-19? Absolutely not. One or all of us may get sick, some may even die. That is the way of things in this life, but this life is not the final chapter, this is only the prelude.
God created this world and the people in it because He is a relational God. He wants people to love and He wants people to love Him as well, but He will never force us into a relationship with Him, because that is not love, that is tyranny. God will allow bad things to happen to us individually, corporately and nationally because it is only through heart ache and suffering that we realize that we cannot do this alone; that we need Him. If things would only go well for us we would think that we are successful by our own efforts and we would never seek or acknowledge His existence or a relationship with Him.
Those of us that have cultivated this relationship with Him and who have accepted the gift of salvation through the sacrifice of Jesus Christ should have a peace about whatever may happen around us. That does not mean that we will never have worries or fears that creep up, nor does it mean that we can act irresponsibly and expect no consequences for our actions, but we should never allow ourselves to become mired in perpetual fear.
2 Timothy 1:7 says “For God has not given us a spirit of fear, but of power, love, and self-control.” As I watch the reactions of people to this virus and the ever changing news around it, I sense that there is a strong spirit of fear at work in society, and that love and self-control are in short supply towards those who have a different view than we have.
I will not be afraid.
It is the fear that causes people to attack others who appear in public without a face mask. It is fear that incites people to wish harm on those who choose to stand up against fear and stand up for the protection of our rights and freedoms that we are all recipients of, not from our governments, but from our creator. Our Charter of Rights and Freedoms is not a list of rights that our government has granted to us, but a list of rights that are not to be infringed upon by any government or any enforcement force for any reason.
There are well meaning Christians that state that we are to obey our government because God has placed that government in its place of leadership, but are we to obey blindly and never question their actions and motives? No! When we see injustice and overreach of authority we are to call our leaders out on it. In the Gospels we are told of Jesus’ own actions against the defilement of the Temple courts under the approval and to the benefit of the leaders of that day, who got wealthy off of the dishonest gains of unscrupulous businessmen who preyed on those that came to worship their God. Jesus overturned the tables, whipped the animals and the people to remove them from the courtyard – He protested! That is our Saviour! That is our example!
Also, in Acts 23 Paul is brought before the Sanhedrin to answer to accusations against him and he calls out the Pharisees and Sadducees on their actions to make them accountable for what they are doing to the Christian believers. The High Priest Ananias ordered that Paul be struck, an absolute abuse of his authority, and Paul challenges the highest leader on his actions and the violation of the laws that the priest is ordained to uphold!
Are these the actions of men who only blindly obey the edicts of corrupt leaders? These men saw injustices and spoke truth to power, the Son of God himself called out the leaders on their corrupted hearts, their insidious actions and their abuse of power! But we have forgotten these examples. We attack each other, believers and unbelievers alike because some are afraid and others refuse to be ruled by fear. Christian brothers and sisters are attacking each other and turning their backs on each other not over theological differences, as bad as that is, but over a tiny virus and whether or not unchristian men are leading us honestly. This is not how it is supposed to be.
I call on all believers to take time to unplug from the news every day and to prayerfully absorb what we are being told, weighing it against long known truths about biology and science. I challenge you all to weigh the value of restrictions that are placed upon us and challenge authority when they are overreaching their responsibilities.
Focus on God, reject fear. We will come through this; it is not worse than other pandemics and is significantly less severe than many. And do not destroy long held relationships will friends and families over something a small as an invisible virus. God calls us to more.
Addendum April 21, 2025: For reference, following is a link to a Whitehouse page that shines some light on the Covid-19 scam well after the fact, highlighting some of the lies and the failures of the so-called professionals that sought to mislead and frighten the public, in my opinion, in order to assert control through fear. Copy and paste this link into your browser to read more.
https://www.whitehouse.gov/lab-leak-true-origins-of-covid-19/
[3] https://www.fda.gov/medical-devices/coronavirus-Covid-19-and-medical-devices/sars-cov-2-reference-panel-comparative-data
[12] https://health-infobase.canada.ca/Covid-19/epidemiological-summary-Covid-19-cases.html?stat=num&measure=tested#a2
[14] https://www.statista.com/statistics/568032/number-of-deaths-in-manitoba-canada/?fbclid=IwAR2w-udtwNDZxlQMG8uWtADzsm__fDPpwKFlVe_tFQBsFwFL1YK8Wf26xr0
[18] https://www.winnipegfreepress.com/special/coronavirus/wire/newsalert-manitoba-makes-masks-mandatory-in-winnipeg-as-Covid-19-cases-surge-572538211.html
[19] https://www.winnipegfreepress.com/special/coronavirus/wire/newsalert-manitoba-makes-masks-mandatory-in-winnipeg-as-Covid-19-cases-surge-572538211.html
[21] https://www.globalresearch.ca/medical-doctor-warns-bacterial-pneumonias-rise-mask-wearing/5725848?fbclid=IwAR1i_Zyi2efx0nKyh0SxqGYQiGIe-HsVtCOnR0XjZzheTo0uMBTgC9SA8Mg
[22] https://www.globalresearch.ca/medical-doctor-warns-bacterial-pneumonias-rise-mask-wearing/5725848?fbclid=IwAR1i_Zyi2efx0nKyh0SxqGYQiGIe-HsVtCOnR0XjZzheTo0uMBTgC9SA8Mg
[23] https://www.msn.com/en-ca/news/canada/aerosol-spread-of-coronavirus-underscores-importance-of-avoiding-e2-80-98three-cs-e2-80-99-tam/ar-BB1aLFtr
[25] https://www.globalresearch.ca/medical-doctor-warns-bacterial-pneumonias-rise-mask-wearing/5725848?fbclid=IwAR1i_Zyi2efx0nKyh0SxqGYQiGIe-HsVtCOnR0XjZzheTo0uMBTgC9SA8Mg



Thank you for writing this so well! All the things I have seen have brought me to the same conclusions. So much data out there if people would look for it. Thanks for listing all the sources as well. I really hope more people will see this and wake up to what is happening.
ReplyDelete